Parasympathetic Component of CN VII: Facial Nerve
Preganglionic parasympathetic axons extend from the superior salivatory nucleus located in the pontine tegmentum and terminate in either the pterygopalatine ganglion, located within the pterygopalatine fossa, or the submandibular ganglion, located slightly inferiorly to the submandibular duct (figure 8).
Pterygopalatine ganglionic fibres:
Submandibular ganglionic fibres:
Pterygopalatine ganglionic fibres:
- Parasympathetic innervation to the lacrimal gland for secretion of tears and the mucous membranes of oral and nasal cavities
- Greater petrosal nerve joins the deep petrosal nerve forming the preganglionic fibres terminating in the pterygopalatine ganglia
- Distributes fibres via the zygomatic nerve, a branch of maxillary division of trigeminal nerve (CN V2) and the lacrimal nerve, a branch of the ophthalmic division of trigeminal nerve (CN V1)
Submandibular ganglionic fibres:
- Preganglionic axons from the chorda tympani branch of CN VII join the lingual nerve, a branch of the mandibular division of trigeminal nerve (CN V3) before terminating in the submandibular ganglion
- Postganglionic axons travel with arteries to salivary glands
- Provides parasympathetic innervation of the submandibular and sublingual salivary glands stimulating the secretion of a watery saliva to aid digestion
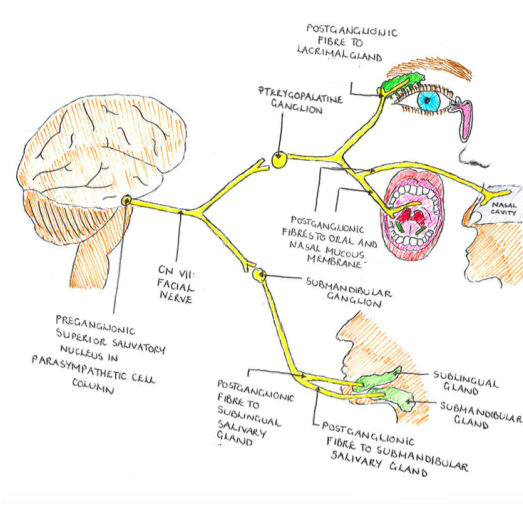
Figure 8. Schematic illustration of preganglionic parasympathetic axons extending from the superior salivatory nucleus in the pons and terminating in either the pterygopalatine ganglion or the sumandibular ganglion. Innervation is subsequently directed to lacrimal glands and oral and nasal mucous membranes for the former, and sublingual and submandibular salivary glands for the latter.
Clinical Implications
Lesions affecting CN VII range from trauma to the parotid region, fractures of the temporal skull, compression following infection and pathologies increasing pressure on the brainstem, such as intracranial haematoma. Due to its extensive pathway, the facial nerve is one of the most commonly injured cranial nerves. Resultant injury depends on the site of the lesion, with the parasympathetic component more severely affected following damage to CN VII near its origin. More centrally located lesions tend to spare lacrimal function.
